
Your Hygienist Has an Hour. Only 30 Are Spent on Hygiene.
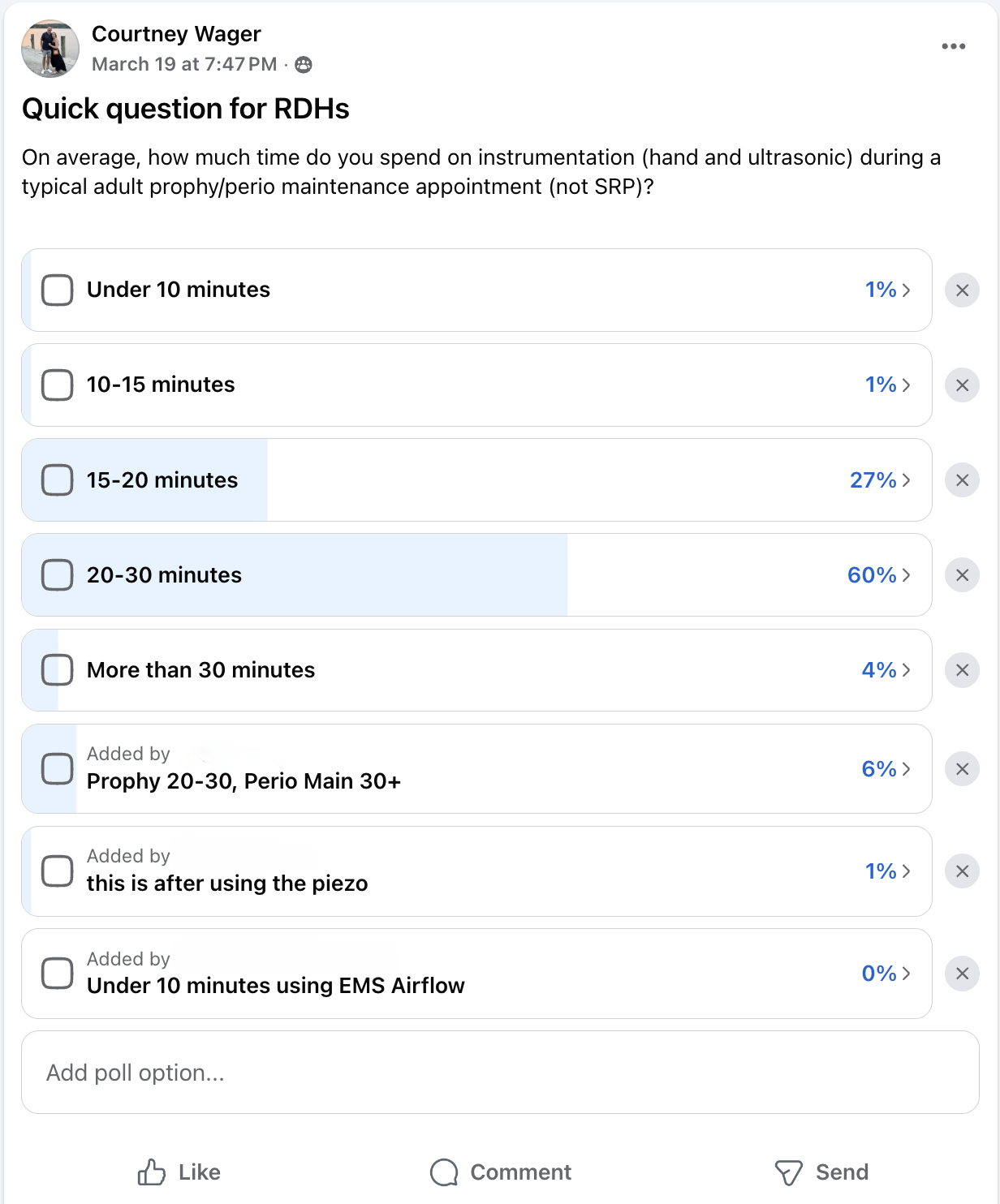
Nearly 90% of hygienists spend 30 minutes or less on instrumentation during a one-hour appointment. So what's filling the other 30 minutes — and does it actually require a hygienist?
Does Thorough Care Require an Hour of Hygienist Time?
Before we answer that, let’s define what most clinicians would probably consider a comprehensive hygiene visit. Pending no time or staffing limitations, most would likely include: a medical history review, radiographs, head and neck/oral cancer screening, periodontal assessment, instrumentation, patient education, polishing/flossing, and doctor exam. Every item on that list happens during my appointments — with about 30 minutes of hygienist time.
Now let me tell you about a patient I saw last week.
While I was finishing up with a patient in one operatory, the assistant I work with seated my next patient in my second room. She took the annual radiographs he needed, updated me on anything important, and got him settled in.
When I walked in, I quickly reviewed the radiographs for anything that stood out. Nothing significant. No medical history changes. Great.
As I started his head and neck screening and opened my instruments, we caught up a bit about his kids and grandkids. Right before I laid him back to begin instrumentation, I asked if anything had been bothering him lately.
He told me that despite wearing a nightguard, he’d been waking up with significant soreness in his TMJ and masseter muscles.
At that point, the focus of the visit changed. Experienced clinicians triage where they can best serve the patient during the time they have.
I asked if he’d ever had a sleep study.
He said yes — five months ago. He’d since been diagnosed with moderate obstructive sleep apnea and was scheduled to review the results with his physician next month.
Five months after diagnosis?! No education, no discussion, and no treatment plan had been communicated to him yet. What an incredible disservice to that patient.
I spent probably twelve minutes discussing how sleep-disordered breathing can contribute to clenching and grinding as the body attempts to open the airway during sleep. We discussed common treatment approaches such as CPAP vs mandibular advancement devices, questions to ask his physician, and what his diagnosis could potentially mean for his longterm health.
The patient was incredibly grateful.
After we covered sleep: I completed instrumentation, performed a Velscope oral cancer screening, wrote my notes, and moved on to see my next patient. Meanwhile, the assistant I work with handled polishing, flossing, dismissal, and recall scheduling. The dentist was not in the office that morning to complete the patient’s periodic exam, so we scheduled him to return for that evaluation on another day.
Assisted hygiene isn’t about seeing double the patients…it’s about removing work that doesn’t require a hygienist.
The single biggest time block reported by hygienists after instrumentation? It’s waiting for the doctor exam. You can see that data here. Comprehensive care does not require a hygienist to independently manage every aspect of the appointment.
Of course, not every patient neatly fits into a 30-minute structure. Complex perio cases, anxious patients, medically compromised patients, and late patients require flexibility. But because there are two of us operating out of two rooms, there’s a buffer for when those unexpected issues arise.
What This Model Has Allowed Me To Do
Working in a two-column assisted hygiene model for nearly twenty years, I am able to provide truly comprehensive care to the patients I treat. I’ve built real relationships with these patients! We talk about their kids graduating, weddings, vacations, and life. Frankly, that’s one of my favorite parts of the job.
I currently see about twelve patients a day. Could I physically see more? Yup. But twelve is what feels sustainable and mentally manageable for me while still allowing me to provide the level of care I’m proud of.
That schedule also allows me to work only three clinical days a week while producing roughly 50% more hygiene production per day than many traditional hygiene models. That serves the practice, and it serves me.
And most importantly — it serves the patient.
Because the doctors I work with have built efficient systems around hygiene. Patients are not sitting around waiting twenty minutes for exams. The assistants and doctors know the flow. The hygienist stays focused on the highest-value clinical aspects of care.
Assisted Hygiene Done Correctly Serves Everyone
It’s not chaos, it’s not double the work, it’s not rushed care.
I’ve worked in this model for twenty years and I haven’t burned out. I’m compensated very well. And I still genuinely love clinical dental hygiene.
When implemented correctly, this model is possible in far more offices than people realize.
If you're a practice owner wondering whether your hygiene department has more capacity than it's currently using, I'm happy to review that with you.